Peer-reviewed articles
Influenza pandemic preparedness in the WHO Eastern Mediterranean Region
Full text
Thematic issue of EMHJ on influenza and other emerging respiratory infections in the Eastern Mediterranean Region
Full Text
Clinical management guidelines for pandemic (H1N1) 2009 virus infection in the Eastern Mediterranean Region: technical basis and overview
Al Hajjar S, Malik MR, Hallaj Z, El-Bushra H, Opoka M, Mafi AR.
Full text [pdf 198kb]
The challenges of global case reporting during pandemic A (H1N1) 2009
Stephanie Williams, Julia Fitzner, Angela Merianos, Anthony Mounts, and for the Case-based Surveillance Evaluation Group
Full Text
Infographics

Key achievements of the Pandemic Influenza Preparedness (PIP) Partnership Contribution implementation in the Eastern Mediterranean Region
Videos
EMARIS 2017 – Interviews and informational videos
Flyers
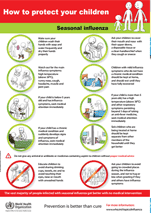
Simple actions can protect you from seasonal influenza
Prevention is better than cure
Data
Global influenza strategy 2019-2030
FluID – a global influenza epidemiological data sharing platform
GISRS – Global influenza surveillance and response System
FluNet – a tool for global influenza virological surveillance
Technical guidance
WHO Global Epidemiological Surveillance Standards for Influenza
WHO checklist for influenza pandemic preparedness planning
WHO collaborating centres and essential regulatory laboratories
Tool for influenza pandemic risk assessment (TIPRA)
Implementation of Pandemic Influenza Preparedness (PIP) in the Eastern Mediterranean Region, July 2014–August 2016
Special issue of the Bulletin on Influenza in the 21st Century Volume 90, Number 4, April 2012, 245-320
Public health measures during the influenza A(H1N1) 2009 pandemic Meeting report
WHO activities in avian influenza and pandemic influenza preparedness January - December 2006
Training materials
Community case management during an influenza outbreak
A training package for community health workers
Meeting reports
Third intercountry meeting on the Eastern Mediterranean Acute Respiratory Infection Surveillance network - Amman, Jordan 14–16 September 2015
Second intercountry meeting on the Eastern Mediterranean Acute Respiratory Infection Surveillance (EMARIS) network - Sharm el-Sheikh, Egypt, 24–27 November 2013
Intercountry meeting on the Eastern Mediterranean Acute Respiratory Illness Surveillance network Sharm el-Sheikh, Egypt 12–13 December 2012
Subregional meeting on improving public health preparedness for epidemic influenza Amman, Jordan 20–22 August 2013
Meeting on influenza at the human-animal interface Cairo, Egypt 19–21 March 2013
Intercountry meeting on Human Pandemic Influenza: establishment/strengthening and alternative strategies for surveillance and response in the Eastern Mediterranean Region, Cairo, Egypt 27–29 April 2010
First consultation of the team of experts on avian and pandemic influenza, Cairo, Egypt 3–7 June 2007
Peer-reviewed articles
Influenza pandemic preparedness in the WHO Eastern Mediterranean Region
Full text
Thematic issue of EMHJ on influenza and other emerging respiratory infections in the Eastern Mediterranean Region
Full Text
Clinical management guidelines for pandemic (H1N1) 2009 virus infection in the Eastern Mediterranean Region: technical basis and overview
Al Hajjar S, Malik MR, Hallaj Z, El-Bushra H, Opoka M, Mafi AR.
Full text [pdf 198kb]
The challenges of global case reporting during pandemic A (H1N1) 2009
Stephanie Williams, Julia Fitzner, Angela Merianos, Anthony Mounts, and for the Case-based Surveillance Evaluation Group
Full Text
Infographics
Key achievements of the Pandemic Influenza Preparedness (PIP) Partnership Contribution implementation in the Eastern Mediterranean Region
Videos
EMARIS 2017 – Interviews and informational videos
Flyers
Simple actions can protect you from seasonal influenza
Prevention is better than cure
Data
Global influenza strategy 2019-2030
FluID – a global influenza epidemiological data sharing platform
GISRS – Global influenza surveillance and response System
FluNet – a tool for global influenza virological surveillance
Technical guidance
WHO Global Epidemiological Surveillance Standards for Influenza
WHO checklist for influenza pandemic preparedness planning
WHO collaborating centres and essential regulatory laboratories
Tool for influenza pandemic risk assessment (TIPRA)
Implementation of Pandemic Influenza Preparedness (PIP) in the Eastern Mediterranean Region, July 2014–August 2016
Special issue of the Bulletin on Influenza in the 21st Century Volume 90, Number 4, April 2012, 245-320
Public health measures during the influenza A(H1N1) 2009 pandemic Meeting report
WHO activities in avian influenza and pandemic influenza preparedness January - December 2006
Training materials
Community case management during an influenza outbreak
A training package for community health workers
Meeting reports
Third intercountry meeting on the Eastern Mediterranean Acute Respiratory Infection Surveillance network - Amman, Jordan 14–16 September 2015
Second intercountry meeting on the Eastern Mediterranean Acute Respiratory Infection Surveillance (EMARIS) network - Sharm el-Sheikh, Egypt, 24–27 November 2013
Intercountry meeting on the Eastern Mediterranean Acute Respiratory Illness Surveillance network Sharm el-Sheikh, Egypt 12–13 December 2012
Subregional meeting on improving public health preparedness for epidemic influenza Amman, Jordan 20–22 August 2013
Meeting on influenza at the human-animal interface Cairo, Egypt 19–21 March 2013
Intercountry meeting on Human Pandemic Influenza: establishment/strengthening and alternative strategies for surveillance and response in the Eastern Mediterranean Region, Cairo, Egypt 27–29 April 2010
First consultation of the team of experts on avian and pandemic influenza, Cairo, Egypt 3–7 June 2007